Private Label, White Label, Wholesale partnerships available - EU, USA and UK - Free shipping from €75
Sterile Laboratory Workflow Guide for Researchers
Discover essential protocols in our sterile laboratory workflow guide to ensure contamination-free results in your research. Click to learn more!
TL;DR:
- A sterile laboratory workflow integrates ISO-compliant engineering controls, disciplined aseptic techniques, and ongoing recertification to prevent contamination. Personnel behavior and proper practices are crucial since human factors most often cause breaches, despite rigorous environment management. Cultivating a culture of operator diligence and stopping work during breaches greatly enhances sterility assurance beyond technical controls alone.
A sterile laboratory workflow is defined as a structured set of protocols, engineering controls, and personnel practices designed to prevent microbial and particulate contamination throughout every stage of a laboratory procedure. This guide addresses the full scope of aseptic technique guidelines, cleanroom best practices, and sterility assurance methods that laboratory professionals need to achieve reproducible, contamination-free results. The frameworks covered here draw from USP <797>, ISO 14644, AORN sterile field principles, and GMP-based biosafety standards. Whether you are managing a compounding facility, conducting peptide research, or operating a biosafety cabinet (BSC) for cell culture work, the protocols in this sterile laboratory workflow guide apply directly to your daily operations.
What cleanroom classifications and engineering controls define sterile lab environments?
Cleanroom classification is the foundation of any laboratory workflow protocol, because the physical environment determines the contamination risk before a single operator enters the space. ISO 14644 establishes the internationally recognized particle concentration limits for each cleanroom class. ISO Class 5 permits a maximum of 3,520 particles per cubic meter at ≥0.5 µm and no more than 29 particles per cubic meter at ≥5.0 µm. These limits define the threshold at which sterile pharmaceutical manufacturing and critical research procedures can be performed with confidence.
| ISO Class | Max particles/m³ (≥0.5 µm) | Typical application |
|---|---|---|
| ISO Class 5 | 3,520 | BSC interior, laminar flow hood |
| ISO Class 7 | 352,000 | Buffer room, compounding anteroom |
| ISO Class 8 | 3,520,000 | General support areas, gowning rooms |
Under USP <797>, the standard governing sterile compounding in pharmaceutical and research settings, a compliant cleanroom layout places ISO Class 5 Primary Engineering Controls (PECs) such as BSCs inside ISO Class 7 buffer rooms, which are accessed through ISO Class 7 or Class 8 anterooms. Pass-through chambers between zones prevent pressure differentials from collapsing when personnel move between areas. This layered architecture means contamination must breach multiple physical barriers before reaching the critical zone.
PEC certification is required before any compounding begins, with recertification scheduled every six months. This interval is not arbitrary. It reflects the rate at which HEPA filter performance, room pressure differentials, and airflow patterns can drift without triggering visible alarms. Recertification at six months catches degradation before it produces a contamination event.
Pro Tip: Document the “at rest” and “operational” particle counts separately during certification. ISO 14644 distinguishes between these two states, and a cleanroom that passes “at rest” may still fail “operational” limits once personnel and equipment are active. Both data sets belong in your quality records.
How do personnel practices and aseptic techniques maintain sterility?
Personnel behavior is the most variable element in any sterile environment practice, and it is also the most frequently cited source of contamination failures. Sterile workflow failures stem more often from human factors than from equipment deficiencies. This finding has direct implications for how laboratories should structure training programs and competency assessments.
The correct sequence for entering a sterile environment follows a defined order that cannot be abbreviated:
- Remove jewelry, cosmetics, and outer garments before entering the anteroom.
- Perform surgical hand antisepsis using a chlorhexidine gluconate or povidone-iodine scrub for the manufacturer-specified duration, typically two to six minutes.
- Don sterile gown, then sterile gloves, in that sequence. Gloving before gowning contaminates the glove exterior.
- Confirm that all PPE is intact and that no skin is exposed at wrist or neck junctions before proceeding into the buffer room or BSC work zone.
- Limit personnel in the sterile area to those directly required for the procedure. Each additional person increases airborne particle load and door-opening frequency.
Sterile field setup should occur as close as possible to the time of use, with only one sterile field open at any given moment. The AORN guideline, originally developed for operating room environments, translates directly to laboratory settings because the underlying contamination physics are identical. A sterile field left open for extended periods accumulates airborne particles regardless of the ISO classification of the surrounding room.
Competency-based training, rather than one-time orientation, is the mechanism that makes aseptic technique second nature. GMP frameworks require documented competency assessments at defined intervals, typically annually and after any procedural change. Laboratories that treat training as a living process rather than a compliance checkbox consistently demonstrate lower contamination rates in environmental monitoring data.

Pro Tip: Conduct unannounced observation sessions where a senior scientist watches a technician perform a full gowning and BSC setup sequence without coaching. Observed deviations during these sessions reveal habitual shortcuts that written assessments never capture.
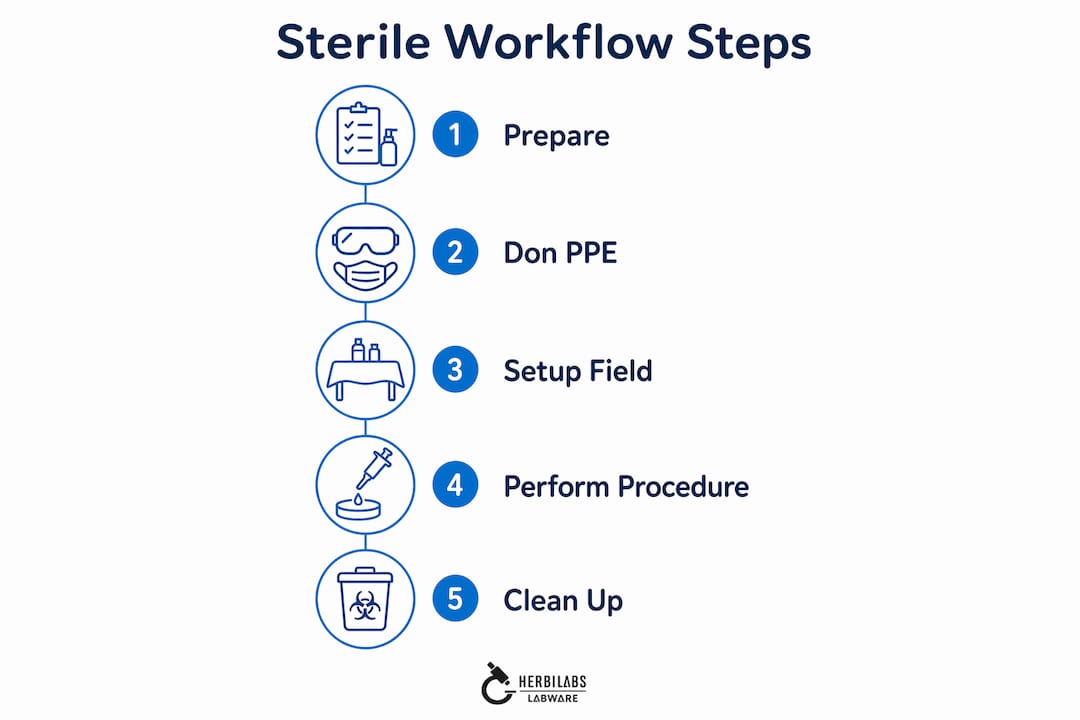
What are the critical workflow steps for executing a sterile procedure?
Executing a sterile laboratory procedure requires a defined sequence that begins before any reagent is opened and continues through final documentation. The following steps represent the core laboratory workflow protocol for BSC-based procedures, applicable to cell culture, peptide reconstitution, and sterile reagent preparation.
- Prepare the environment. Disinfect the BSC interior with 70% isopropyl alcohol or a validated sporicidal agent at least 15 minutes before work begins. Allow the BSC blower to run for a minimum of five minutes after disinfection to purge residual aerosols.
- Organize materials before opening sterile packaging. Arrange all consumables, reagents, and waste containers within the BSC before breaking any sterile seal. Reaching in and out of the BSC after work begins is the primary mechanism by which airflow disruption introduces contamination.
- Open sterile packaging at the BSC front edge. Peel packaging away from the sterile item rather than tearing across it, and deposit items directly onto the sterile field without touching the interior of the packaging to any non-sterile surface.
- Work from clean to contaminated. Process the lowest-risk samples first. If working with multiple reagent vials, handle unopened, sterile vials before any previously accessed containers.
- Minimize movements inside the BSC. Slow, deliberate arm movements parallel to the work surface preserve laminar airflow. Rapid or lateral movements create turbulence that pulls room air into the ISO Class 5 zone.
- Address contamination breaches immediately. Stop work to assess breaches rather than continuing cautiously. A “continue with caution” response to a suspected breach is not an acceptable corrective action under any recognized sterility assurance framework.
The table below compares two common workflow configurations used in sterile laboratory settings:
| Workflow type | Airflow model | Best suited for | Key limitation |
|---|---|---|---|
| Unidirectional laminar flow | Horizontal or vertical HEPA-filtered flow | Sterile reagent prep, compounding | Operator must not obstruct airflow path |
| Adapted open-bench layout | Ambient air with localized BSC | General microbiology, cell culture | Higher contamination risk outside BSC zone |
Pro Tip: When handling lyophilized peptides or other hygroscopic compounds, pre-warm the vial to room temperature inside the sealed container before opening it inside the BSC. This prevents condensation on the vial interior, which can compromise reconstitution accuracy and introduce moisture-related degradation.
How to troubleshoot common challenges in maintaining sterile workflows
The most frequent errors in sterile laboratory workflows are predictable, and most trace back to a small number of root causes. Understanding these failure modes allows laboratories to design preventive controls rather than reactive responses.
- Premature sterile field setup. Opening sterile packaging significantly before the procedure begins increases particle deposition on exposed surfaces. The sterile field timing principle from AORN specifies that setup should occur immediately before use. In practice, this means completing all non-sterile preparation steps first, then opening sterile items in sequence as they are needed.
- Uncontrolled door openings. Each door opening between the anteroom and buffer room creates a pressure pulse that temporarily disrupts the directional airflow maintaining ISO class separation. Laboratories should log door opening frequency as part of environmental monitoring and investigate any procedure that requires more than two entries per session.
- Delayed recertification after facility changes. Recertification must occur whenever changes affect airflow or air quality, not only on the six-month schedule. HVAC filter replacements, equipment relocation, and even ceiling tile repairs qualify as triggers. Laboratories that treat recertification as a calendar event rather than a risk-responsive process accumulate undetected performance drift.
- Inadequate environmental monitoring frequency. Surface sampling, air sampling, and personnel monitoring should occur at a frequency proportional to the risk level of the work performed. ISO Class 5 environments used for sterile compounding require more frequent monitoring than ISO Class 7 support areas.
“Workflow discipline in operator behavior is as important as engineering controls for maintaining sterility. Physical disinfectants alone are insufficient if airflow is disrupted by improper movements inside biosafety cabinets.”
— NCBI Biosafety Guidelines
Quality management integration is the mechanism that converts individual corrective actions into systemic improvement. Laboratories that link environmental monitoring data to training records, and that review both during periodic quality meetings, identify recurring human factors before they produce reportable contamination events. For further detail on contamination breach responses and corrective action documentation, structured protocols are available that align with GMP expectations.
Key takeaways
A sterile laboratory workflow requires the integration of ISO-compliant engineering controls, disciplined aseptic technique, and event-responsive recertification to sustain contamination-free conditions across all procedure types.
| Point | Details |
|---|---|
| ISO Class 5 is the critical threshold | PECs must meet ≤3,520 particles/m³ at ≥0.5 µm before any sterile work begins. |
| Recertify on schedule and after changes | USP <797> requires recertification every six months and after any airflow-affecting facility modification. |
| Sterile field timing is non-negotiable | Open sterile packaging immediately before use and limit active sterile fields to one at a time. |
| Human factors drive most failures | Training embedded in work culture reduces contamination errors more effectively than checklist enforcement. |
| Stop work on any suspected breach | Continuing cautiously after a contamination event is not an acceptable response under any recognized sterility assurance standard. |
Why engineering controls alone will never be enough
Having spent considerable time reviewing contamination investigation reports from research and compounding environments, one pattern appears with striking consistency: the cleanroom passed certification, the BSC was disinfected on schedule, and the contamination event still occurred. The root cause, in the majority of these cases, was an operator movement. A hand withdrawn too quickly from the BSC. A door opened mid-procedure to retrieve a forgotten item. A sterile field left open while the technician stepped away to answer a question.
This is not a criticism of the operators involved. It reflects a structural problem in how many laboratories approach sterile environment practices. The engineering controls receive rigorous documentation and scheduled verification. The operator behavior receives an annual training module and a signature on a competency form. The asymmetry between these two levels of rigor is where contamination risk accumulates.
What I have found actually works is treating aseptic manufacturing discipline as a behavioral standard rather than a procedural checklist. The laboratories with the lowest contamination rates are not necessarily those with the most sophisticated cleanrooms. They are the ones where stopping work to assess a suspected breach is genuinely normalized, where no one feels pressure to continue cautiously because the batch is time-sensitive. That cultural standard is harder to build than an ISO Class 5 environment, and it is far more difficult to certify. But it is the variable that most reliably separates laboratories with consistent sterility records from those with recurring incidents.
The other observation worth stating directly: USP compliance is a floor, not a ceiling. Meeting the six-month recertification interval and the particle concentration limits is the minimum required to operate. Laboratories that treat compliance as the target rather than the baseline will find that their quality data reflects exactly that level of ambition.
— Ragnar
Sterile reagents and reconstitution solutions from Herbilabs
Maintaining a sterile laboratory workflow depends not only on your protocols and environment, but also on the quality of the reagents and reconstitution solutions you introduce into that environment. A single contaminated diluent can compromise an entire sterile field regardless of how precisely your cleanroom is managed.
Herbilabs manufactures high-purity reconstitution solutions in a dedicated facility under strict quality control standards, producing sterile diluents and bacteriostatic water suitable for demanding research environments. Each product is manufactured to research-grade purity specifications, with contaminant-free formulation verified before release. For laboratories working with lyophilized peptides or other sensitive compounds, Herbilabs also provides guidance on selecting the right reagents to match your specific reconstitution requirements. Explore the full product range to find solutions that integrate directly into your existing sterile workflow protocols.
FAQ
What is the ISO class required for sterile compounding?
USP <797> requires an ISO Class 5 environment inside Primary Engineering Controls such as biosafety cabinets for all sterile compounding procedures. The surrounding buffer room must meet ISO Class 7 standards.
How often must cleanrooms be recertified under USP <797>?
Cleanrooms and PECs must be recertified every six months under USP <797>. Recertification is also required after any facility change that affects airflow or air quality, including HVAC modifications or equipment relocation.
What is the correct sequence for donning PPE before entering a sterile lab?
Surgical hand antisepsis is performed first, followed by gowning, then gloving. Reversing this sequence contaminates the glove exterior and compromises the sterile barrier before work begins.
What should you do if a sterile field is breached during a procedure?
Work must stop immediately to assess the breach. Continuing cautiously after a suspected contamination event is not an acceptable corrective action under AORN guidelines or GMP-based sterility assurance frameworks.
Why does unnecessary movement inside a BSC cause contamination?
Rapid or lateral arm movements inside a biosafety cabinet disrupt the laminar HEPA-filtered airflow that maintains ISO Class 5 conditions. This turbulence draws ambient room air into the critical zone, introducing particles and potential contaminants to the sterile field.